 The scientific literature has started to build that runners with knee osteoarthritis can, and perhaps should, continue to run without the fear of significant worsening of their knee joint. The medical professions have often tried to dissuade people from running with the presumption that a high impact activity was likely to cause worsening of the patients arthritis. Most runners love their sport and have no desire to trade in prematurely for an activity considered low impact. The news that you need to find a new activity can be traumatic for this very committed group of athletes. The cardiovascular and mental benefits of running are well understood and this is what has led to further studies to ensure that the medical profession is giving the right advice to the patient group presenting with knee arthritis.
A recent study (Lo GH in Clinical Rheumatology 2018) looked at the effects of “self selected” running in a group of over 50 year old runners. Self selected running really describes running at a speed and distance on a regular interval that the runner determines is unlikely to significantly aggravate their knee pain. Every participant had to have Osteoarthritis in at least one knee joint. Assessment of the study was made through repeat radiographs and various knee assessment questionnaires completed by the patients over a 48 month period. The results of the study demonstrated no increase in radiographic progression of the arthritis and an improvement in knee pain rather than worsening of knee pain. I would also be confident that if other factors both physiological (eg: blood pressure, heart rate and BMI) and psychological were considered, that we most likely would have seen improvements in these areas as well. So the take home message – those of us diagnosed with OA of the knees can probably still run but it must be at your own pace and distance (self selected) and this may be variable day to day. I would also still suggest a review with a physiotherapist to ensure that you don't have anything more serious that might preclude you from a return to running. Otherwise get out there and get running. The words and other content provided in this blog and in any linked materials, are not intended as medical advice and are an opinion only. If the reader or any other person has a medical concern you should consult a medical practitioner immediately. While Physiosense Physiotherapy have made every effort to ensure the information supplied on this web site is suitable, accurate and complete, we accept no responsibility for any loss or liability incurred by any party as a result of accessing or utilising the information on this website, blog or for any websites linked to or from this website. We try to ensure the information on this website is up-to-date and accurate, however we take no responsibility for inaccuracies or any information that is out of date. THIRD PARTY CONTENT/LINKS Any opinions, by any third parties within or linked to this website such as statements, articles uploaded or other information or content expressed or made available are those of the respective author(s) and not necessarily those of Physiosense Physiotherapy. There is good evidence that early referral to scanning for a patient with lower back pain is correlated with a poorer reduction in overall reported pain, and a longer recovery time (Ref: 1). It is also well known that asymptomatic individuals can have significant changes noted on scans (Ref : 2) that are better described as normal age related changes. But let's consider that you have had your scans and they describe a bulge, an extrusion, herniation or protrusion, and this picture has you very worried about the chances of a good non-surgical recovery. The question must be asked, “Can these disc changes reduce with more conservative actions, or is surgery required “?edit. Concisely the answer is yes, that both clinically (ie: in practice) and academically(using repeat MRI's to review disc changes over time- Ref : 3 and 4), significant resolution of disc bulges and patient symptomology occurs with conservative treatment.
Sometimes surgery is required but increasingly it appears that more conservative measures such as physiotherapy and time, are being prescribed under certain circumstances, even in patients with quite severe presentations. The mechanisms as to why these disc changes can resolve is not completely understood, especially when mechanical loading or compression of the disc may oppose this process ( Ref : 5 ). One explanation is autolysis, which basically describes an autoimmune process whereby extruded disc tissue and inflammation, is recognised by macrophage cells and resorbed into the body. This leads to a reduction of the appearance of the disc herniation/disruption on MRI and decreased irritation of the spinal cord and nerves. This blog does not attempt to provide a pathway for making a decision about the treatment of lower back pain but rather to provide hope, that conservative measure can be effective even for patients with more severe presentations. A full assessment by a qualified Physiotherapist or Doctor needs to be considered before appropriate management can be implemented. Treatment decisions for lower back pain are more complex than described above and the signs, and symptoms must be recognised for all of the other possible pathologies of the spine for better treatment of the patient.......our focus at Physiosense. 1: Of shiny pictures and poorer outcomes: Spinal MRI and back pain https://bodyinmind.org/spinal-mri-and-back-pain/ 2: Systematic Literature Review of Imaging Features of Spinal Degeneration in Asymptomatic Populationshttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC4464797/ 3:Spontaneously disappearinglumbardisc protrusionhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC2529204/ 4: Spontaneous Regression of a Large Lumbar Disc Extrusionhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC2966735/ 5: Conservatively treated massive prolapsed discs: a 7-year follow-up https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3025225/ The words and other content provided in this blog and in any linked materials, are not intended as medical advice and are an opinion only. If the reader or any other person has a medical concern you should consult a medical practitioner immediately. While Physiosense Physiotherapy have made every effort to ensure the information supplied on this web site is suitable, accurate and complete, we accept no responsibility for any loss or liability incurred by any party as a result of accessing or utilising the information on this website, blog or for any websites linked to or from this website. We try to ensure the information on this website is up-to-date and accurate, however we take no responsibility for inaccuracies or any information that is out of date. THIRD PARTY CONTENT/LINKS Any opinions, by any third parties within or linked to this website such as statements, articles uploaded or other information or content expressed or made available are those of the respective author(s) and not necessarily those of Physiosense Physiotherapy.  In the world of rehabilitation/physiotherapy cycling is often prescribed as a great way to build quads strength without aggravating sore and painful joints. Mostly this is true but even in the good knee cycling can also cause pain if your cycle training is not approached in the correct way. The attached article has some great ideas, certainly many points relevant to patients that I have seen in the clinic and on the bike. Good luck and enjoy your cycling, painfree of course. http://www.bicycling.com/…/7-ways-youre-hurting-you…/slide/3 The words and other content provided in this blog and in any linked materials, are not intended as medical advice and are an opinion only. If the reader or any other person has a medical concern you should consult a medical practitioner immediately. While Physiosense Physiotherapy have made every effort to ensure the information supplied on this web site is suitable, accurate and complete, we accept no responsibility for any loss or liability incurred by any party as a result of accessing or utilising the information on this website, blog or for any websites linked to or from this website. We try to ensure the information on this website is up-to-date and accurate, however we take no responsibility for inaccuracies or any information that is out of date.
THIRD PARTY CONTENT/LINKS Any opinions, by any third parties within or linked to this website such as statements, articles uploaded or other information or content expressed or made available are those of the respective author(s) and not necessarily those of Physiosense Physiotherapy. The results of the recent study published in the Australian medical Journal regarding efficacy of Acupuncture in treatment of low back pain and ankle sprains has added weight to what a lot of physiotherapists have been seeing in General practice. The study was a randomised control trial of high quality with the data collected from four major Australian hospitals.
The study looked at acupuncture versus acupuncture and medication, versus medication only, in the acute treatment of migraines, lower back pain and ankle sprain. At my clinic I don’t use it on everybody and certainly not on anyone who has any fear or general dislike of needles. Applying acupuncture to the right patient at the right time has achieved some great results. The Study Outline: 1,964 patients took place in the four centre study. A verbal rating scale out of ten (ten being excruciating pain and zero being no pain) with a score of four or above was needed for the patient to participate in the study. A meaningful change was noted as two points difference on the scale. One hour after treatment less than 40 percent of patients across all groups experienced greater than 2/10 in pain relief with 80 percent still acknowledging pain of 4/10 or more. “But 48 hours later, the vast majority found their treatment acceptable, with 82.8 per cent of acupuncture-only patients saying they would probably or definitely repeat their treatment, compared with 80.8 per cent in the combined group, and 78.2 per cent in the pharmacotherapy only group” - Science Daily. To summarise, all groups provided a nearly equivalent level of relief at the one hour and forty-eight hour measures therefore acupuncture can be considered as an effective treatment for pain relief in the acute setting. Further considerations of safety and pain management in general are succinctly noted in these paragraphs from Science Daily - "Emergency nurses and doctors need a variety of pain-relieving options when treating patients, given the concerns around opioids such as morphine, which carry the risk of addiction when used long-term. Our study has shown acupuncture is a viable alternative, and would be especially beneficial for patients who are unable to take standard pain-relieving drugs because of other medical conditions. But it's clear we need more research overall to develop better medical approaches to pain management, as the study also showed patients initially remained in some pain, no matter what treatment they received." https://www.sciencedaily.com/releases/2017/06/170618103517.htm https://www.mja.com.au/journal/2017/206/11/acupuncture-analgesia-emergency-department-multicentre-randomised-equivalence The words and other content provided in this blog and in any linked materials, are not intended as medical advice and are an opinion only. If the reader or any other person has a medical concern you should consult a medical practitioner immediately. While Physiosense Physiotherapy have made every effort to ensure the information supplied on this web site is suitable, accurate and complete, we accept no responsibility for any loss or liability incurred by any party as a result of accessing or utilising the information on this website, blog or for any websites linked to or from this website. We try to ensure the information on this website is up-to-date and accurate, however we take no responsibility for inaccuracies or any information that is out of date. THIRD PARTY CONTENT/LINKS Any opinions, by any third parties within or linked to this website such as statements, articles uploaded or other information or content expressed or made available are those of the respective author(s) and not necessarily those of Physiosense Physiotherapy.
The words and other content provided in this blog and in any linked materials, are not intended as medical advice and are an opinion only. If the reader or any other person has a medical concern you should consult a medical practitioner immediately. While Physiosense Physiotherapy have made every effort to ensure the information supplied on this web site is suitable, accurate and complete, we accept no responsibility for any loss or liability incurred by any party as a result of accessing or utilising the information on this website, blog or for any websites linked to or from this website. We try to ensure the information on this website is up-to-date and accurate, however we take no responsibility for inaccuracies or any information that is out of date.
Just a short blog to discuss recovery after tendinopathy and how it's all about appropriate loading, not too much or too little. This is a great diagram to explain just what this means ie: what is acceptable and in what time period after your effort. You still need to be patient as tendons can take some time to heal but information like this does allow you to manage a gradual return to sport in a safer way. Tendinopathy can be difficult to treat and the damage or recovery of your tendon should be assessed by a qualified physiotherapist. 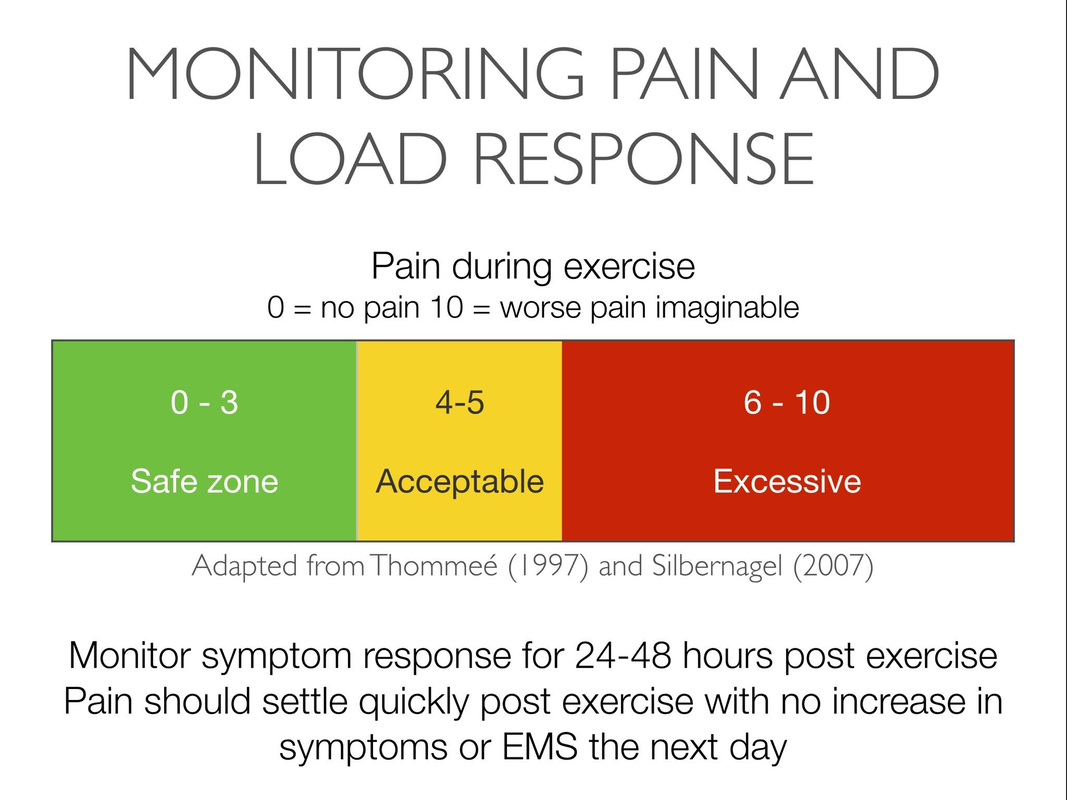 The words and other content provided in this blog and in any linked materials, are not intended as medical advice and are an opinion only. If the reader or any other person has a medical concern you should consult a medical practitioner immediately. While Physiosense Physiotherapy have made every effort to ensure the information supplied on this web site is suitable, accurate and complete, we accept no responsibility for any loss or liability incurred by any party as a result of accessing or utilising the information on this website, blog or for any websites linked to or from this website. We try to ensure the information on this website is up-to-date and accurate, however we take no responsibility for inaccuracies or any information that is out of date.
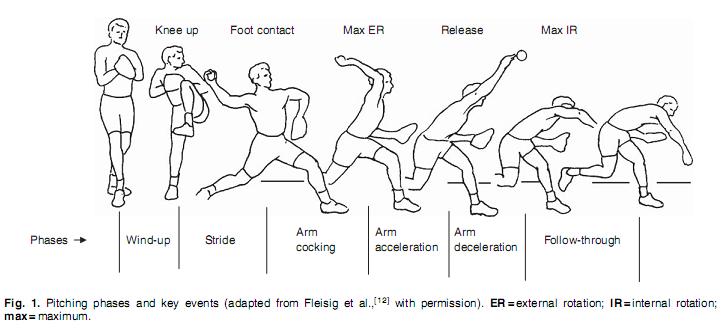 As we move into summer our sports tend to become a little more throwing orientated so I felt that it would be a good chance to consider a few factors predisposing the sports person to a throwing injury. I recently reviewed an excellent blog; https://mikereinold.com/gird-baseball-pitching-injury/ which prompted my review. It was really refreshing to see some experts describe that they were not better than everybody else at their assessments but that they have the opportunity to see many more throwing injuries and therefore have a better idea of what to consider. A small blog is not going to cover the many injuries of the upper limb that occur from throwing but hopefully it can give enough information to prompt a review when you think that you might be out of your depth. 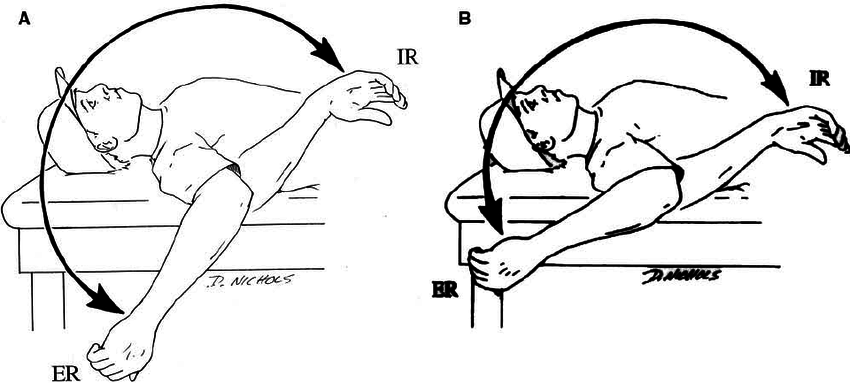 The review article (by Lenny Macrina)describes an internal rotation deficit being traditionally correlated with an increased incidence of shoulder injuries. This made me consider a seminar with a prominent Australian physio a few years ago who commented that he felt it was the total range of combined internal and external rotation that mattered more than just an internal rotation deficit. Indeed by the end of the article Lenny has largely drawn the same conclusions. So the overall consideration of the throwing athlete is much more than just a simple assessment of range. At the speed a hard throw is released our biomechanics have to be well aligned so that we do not cause increased stress on any of the body tissues related to this motion. Classically in Australia this most closely relates to our cricketing fast bowlers that seem to get small but debilitating injuries as they push themselves to their biomechanical limits. The body is just working on the edge of what is possible. So its not just about increased flexibility or range because this can quickly descend into laxity and injury. A further example is the consideration of external rotation. External rotation is often considered crucial in developing arm speed as it is important in the cocking motion of the throw and helps the thrower develop more speed as the arm moves into position to release the ball by forcefully internally rotating the shoulder. A blog by Tread Athletics :”Do you need 180+ degrees to throw harder? No”;describes that pro baseball pitchers in America tend to have between 160 to 185 degrees of external rotation so other factors must be considered in determining overall ball speed http://treadathletics.com/blog/external-rotation-throw-harder/. The Tread Athletics blog also develops some excellent training principles for consideration of the whole biomechanical chain, from lower body strengthening of the gluteals then back up to mobilising the thoracic spine. If you need any more convincing have a look at these “fun” facts from https://www.p2sportscare.com/shoulder-pain-pitching/ : Fun Facts on Shoulder Pain while Pitching Fact #1:13%: The percentage of the force generated by the shoulder when pitching. (9,10,11,26)Notice that this is not a large percentage at all. This means that much your velocity in pitching will does not come from the arm/shoulder. So then where does it come from? See the fact below to find out. Fact #2:51-55%: The percentage of force generated by the trunk, pelvis, and legs when pitching. (9,10,11,26)This percentage is huge! The power that your lower body produces is where most of your pitching velocity comes from. Great pitchers don’t just glide off the mound, they drive off the mound. By using your lower body more during pitches, you could just end up saving your shoulder and elbow from a lot of pain and frustration later on. Throwing is complex when you break it down, if your starting to get pain with this activity its probably times to see a physio for a proper clinical review. A few exercises to get you started:
Get your summer started right and don't just get out there and expect to start where you finished last season. Our bodies adapt quickly and you cant expect your throwing to be as strong if you haven’t continued this activity during the off season. The words and other content provided in this blog and in any linked materials, are not intended as medical advice and are an opinion only. If the reader or any other person has a medical concern you should consult a medical practitioner immediately. While Physiosense Physiotherapy have made every effort to ensure the information supplied on this web site is suitable, accurate and complete, we accept no responsibility for any loss or liability incurred by any party as a result of accessing or utilising the information on this website, blog or for any websites linked to or from this website. We try to ensure the information on this website is up-to-date and accurate, however we take no responsibility for inaccuracies or any information that is out of date.
After completing the Science of Cycling course recently, I have a much greater understanding of the importance of a good bike fit for comfortable and powerful cycling. This seems logical enough but it surely isn’t where it all stops. Just think of the “ergonomic” workplace assessment. You just got the perfect monitor and desk height, your chair is perfect but your discomfort may not be completely resolved. Could the ergonomic assessment be wrong? I feel that this sometimes is not the case. As with a bike fit, when fitting someone to their workplace we use certain suggested parameters or guidelines, so really it's about finding a good baseline set-up and working with it, rather than accepting yours as the perfect arrangement. So if you slip into slumping at your desk, then your assessment fails to matter and the same can be said of good riding posture. Once you are set-up in a good position, not just that perfect pedalling and positioning found/applied by the bike fitter on your day in the shop, but are able to maintain this position out on the track, then you will feel the benefits . So where do we start with my latissimus dorsi experience ? Firstly, my list of problems riding my mountain bike included numb hands, occasional back ache and some pelvic soreness. My bike fit was pretty good so it wasn’t making much sense that I had these problems. I feel that two things helped to improve my cycling experience.
And there you have it. By gaining a better position over the saddle, losing the monkey arms and changing my pedalling position, I have been able to eliminate aches that I was experiencing after some longer rides. I try to keep the blogs short but if you want some extra detail I have attached an excellent reference article below, and if you're still struggling then book in for a bike fit/cycling review at physiosense where I'll be glad to help. https://www.teamusa.org/USA-Triathlon/News/Blogs/Multisport-Lab/2015/December/08/Posture-Perfect-Exercises-for-a-Strong-Cyclist. The words and other content provided in this blog and in any linked materials, are not intended as medical advice and are an opinion only. If the reader or any other person has a medical concern you should consult a medical practitioner immediately. While Physiosense Physiotherapy have made every effort to ensure the information supplied on this web site is suitable, accurate and complete, we accept no responsibility for any loss or liability incurred by any party as a result of accessing or utilising the information on this website, blog or for any websites linked to or from this website. We try to ensure the information on this website is up-to-date and accurate, however we take no responsibility for inaccuracies or any information that is out of date.
Initially considered as part of a warm up routine, there does also appear to be performance benefits from completing the program regularly. Compliance is key with the program needing to be competed in full, 2-3 times per week and the running components of the program only being completed prior to a match. A full review of all of the noted information can be found at https://bjsm.bmj.com/content/49/9/577 ACL injuries unfortunately are not completely unavoidable but there is good evidence that the Fifa 11 Plus program helps to significantly decrease the amount of injuries suffered by a team/club cohort in a season. Some studies suggest up to a 50% reduction in injuries to females and potentially 40% in males. Some more recent studies also outline success in other sports such as Basketball. More explicit information on the technical positioning of the player can be found at the link below or on review with a physiotherapist with experience of the program. http://www.yrsa.ca/pdf/Fifa11/11plus_workbook_e.pdf The words and other content provided in this blog and in any linked materials, are not intended as medical advice and are an opinion only. If the reader or any other person has a medical concern you should consult a medical practitioner immediately. While Physiosense Physiotherapy have made every effort to ensure the information supplied on this web site is suitable, accurate and complete, we accept no responsibility for any loss or liability incurred by any party as a result of accessing or utilising the information on this website, blog or for any websites linked to or from this website. We try to ensure the information on this website is up-to-date and accurate, however we take no responsibility for inaccuracies or any information that is out of date.
Not having the correct breast support while running leads to discomfort, which in turn is leading to some women avoiding running altogether, according to Dr Deirdre McGee and her colleagues at the University of Wollongong. I recently attended a running symposium with Sports Medicine Australia and one of the topics on the agenda was Bra fitting. I found it interesting that the studies found that it was not only large breasted women that benefited from a better fitting bra. A comment made by one of the smaller breasted women participating in one of the studies sums this up as she describes that she was happy running and didn't have pain, but her newly fitted bra made her running “so much more comfortable”. Another stated that she found running painful and this impacted directly on how much running she could complete. After a correct fitting she had much less pain with this activity and progressed to lose 10Kg as she was able to increase her running distances. Basically it seems that physics has a large part to play, and the stress on breast tissue is not only affected by weight but by how many cycles (i.e. superior to inferior movements in the case of breasts during running) that are applied. Breast Research Australia has developed an App that contains “evidenced based information to ensure the next bra you buy is the right size, is supportive and most importantly is comfortable”. The App can be freely downloaded from www.bra.edu.au/sportsbra. Much of this information was gained through the clinical research efforts of Dr Deirdre McGee and her colleagues. Deirdre has also been involved in developing guidelines for Sports Medicine Australia which can be downloaded in the form of the brochure exercise and breast support from the link below. As a male I found it astounding that there could be so many variations in design of the bra. Its not just simply good wire and strong elastic, or that all designs work with all women. Good luck with the App, I hope it helps to take some of the pain out of your activities and indeed bra selection. The words and other content provided in this blog and in any linked materials, are not intended as medical advice and are an opinion only. If the reader or any other person has a medical concern you should consult a medical practitioner immediately. While Physiosense Physiotherapy have made every effort to ensure the information supplied on this web site is suitable, accurate and complete, we accept no responsibility for any loss or liability incurred by any party as a result of accessing or utilising the information on this website, blog or for any websites linked to or from this website. We try to ensure the information on this website is up-to-date and accurate, however we take no responsibility for inaccuracies or any information that is out of date. |
AuthorJason is the Leichhardt Physiotherapy clinic practice principal. A graduate from Sydney Uni and practicing for over 20 years, he is passionate about sharing new discoveries. |

 RSS Feed
RSS Feed